

Burns are injuries which are predominantly to the skin and superficial tissues (adipose). Burns can be caused by several external factors such as the sun, fire, hot materials and even extremely cold materials. In extreme cases, burns can even affect the bones through high voltage electrical injury.
Assessment:
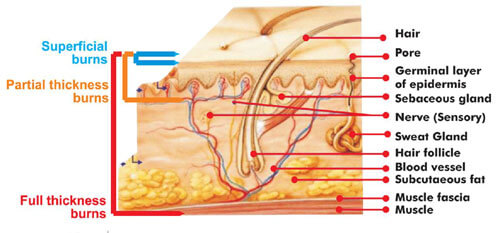
The severity of the burn is assessed through depth or thickness, surface area and location.
In terms of depth or thickness, there are varying degrees of burns including superficial, partial and full thickness.
To assess surface area, the rule of nines method is predominantly used:
- The head and neck represent 9%
- Each upper extremity represents 9%
- Each lower extremity represents 18%
- The anterior and posterior torso represent 18% each
- The genital area represents 1%
- Due to the size of infants and children, the percentages are different.
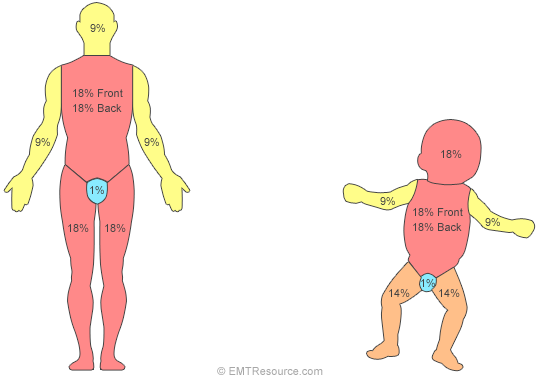
TIP: The palm of the victim’s hand represents approximately 1% of their body surface area.
In terms of location, if there are burns to the airway or torso, this can negatively affect ventilation.
PLEASE NOTE: Airway stability should be assessed as a priority in burns to the face or where there is suspicion of inhalation injuries. Burns to the airway and inhalation injuries are life-threatening.
Management:
Remove the patient from any immediate danger and use the Basic Life Support Chain to ensure they have an open and clear airway, normal breathing and sufficient circulation.
As burns can reduce the body’s blood volume, it is critical to monitor the patient for signs of hypovolemic shock. If the patient is displaying symptoms of shock (pale, cool & clammy skin), this is a medical emergency and the patient should be placed in the recovery position if they’re unconscious or flat on their back if they are conscious. As gravitational forces have a significant influence on the venous return to the heart, placing the patient in a horizontal position is very advantageous.
Once the patient is hemodynamically stable (the patient has sufficient blood flow around the body and is breathing normally), the cooling process should begin. The best treatment for a burn is cool, running water for approximately twenty minutes. It is important that this is not done until the patient is stable- there isn’t any point in cooling a burn when the patient isn’t breathing.
After the cooling process, the burn should be wrapped in a loose cling film layer, unless the burn was caused by a chemical. This prevents the outside air from irritating the nerve receptors. This will ultimately reduce pain sensation and prevent further contamination.
Myths:
- DO NOT USE ICE OR ICE WATER TO COOL THE BURN
- DO NOT USE TOMATOES, MAYONNAISE OR BUTTER TO COOL THE BURN
- DO NOT POP OR BURST BLISTERS
- DO NOT REMOVE CLOTHING OR JEWELLERY WHICH HAS ADHERED TO THE BURN
Impact of Management:
Initial management for patients suffering from burns, aims to protect them from ongoing injury, stabilise their system and transport them to a sterile environment for definitive treatment (such as a hospital). Healing of burns is typically a long and painful process which can have long lasting psychological consequences for the patient. It is important that these are addressed in the overall management of the patient. It is inevitable that the patient will have some form of scarring, irrespective of attempts made by a multidisciplinary team to minimise these affects. A high priority should be given to protecting the patient from infection, in order to avoid demise due to sepsis (life threatening condition caused by the body’s response to an infection.)